Small screw anchors currently available on the market tend to be made with finer needles and suture material. We have designed an anchor specifically for the foot and ankle in which the thread and suture strength has not been compromised. Our Ultrapoint needle is sharper and stronger than competitors allowing penetration through the strong joint capsules encountered in the foot. The stronger fibre wire potentially allows earlier rehabilitation, weight bearing and return to sporting activities.
Tendon and Ligament Repair
Super strong pull out strength
Fibrewire suture
Hard needles
Easy to use
SMALL
3500 N Pull Out
Brostrum
Metatarsal
Wrist
LARGE
5000 N Pull Out
Shoulder
Knee
Self tapping screw
INDICATIONS
This product is designed for use in tendon and ligament repair surgeries. Ultra point needles can penetrate through strong capsule and ligaments.
Anchor: Corkscrew Drill Dimension: 3.5mm x 12.5mm Suture Size: 2 Number of Sutures: 4 Ultrapoint needles with Klotho fiber #2 UHMWPE Drill Type: Self Tapping Material: Titanium Order Code: SSA-3500N Anchor Drill: 2.0mm x 100mm, 3.0mm x 100mm Order Code: AD-350
Pearls & Pitfalls
Ultrapoint needle strength allows for larger purchase “bites” of capsule.
The more generous thread gives superior pull out strength.
BE CAREFUL with drill preparation. Strong bone requires a larger preparation hole. The 3mm reamer may need to be toggled at the entrance to allow this when bone is hard.
If anchor is not fully inserted the handle can be placed back over the anchor and insertion completed. If interference greater than handle strength either remove anchor with small lambotti or drilling around it with pilot reamer or impact with punch.
Design Rationale
This product features a titanium corkscrew anchor with ultra-high molecular weight polyethylene suture (fibre). Disposable insertion tool consists of handle and stainless steel. The implant is designed to pass through the ropes. The anchor is a fully threaded corkscrew design to obtain maximum purchase and hold in soft cancellous bone. The corkscrew anchor is available in 3.5mm and 5.0mm dimensions.
Fully Threaded Design
Pulling Strength
Self tapping Screw Design
Easy Implantation
Easy Floating Needles with Special Design Suture
MODIFIED BROSTRUM
Reconstruction
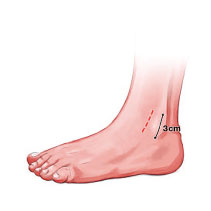
Ankle Arthroscopy Incision placement is anterior border of the fibula, 3cm incision. Blunt dissection down to the lateral capsule.
Diathermy of Bleeding Points The lateral capsule is divided with sharp dissection. The fibula wall exposed and the anchor insertion points identified. A flap of tissue is mobilised over the fibula.
The Lateral Ligaments are not dissected as distinct anatomical structures . Rather the lateral wall is mobilised as a cuff.
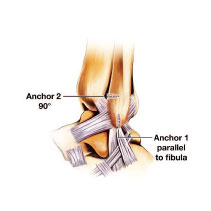
The Anchors are inserted into the fibula. Integrant 3.5 mm anchors are used. A blue bone sparing reamer is used and drilled the depth of the anchor. The anchors havea coarse thread and are self drilling in most bone. However if they are inadequately reamed they may become stuck.
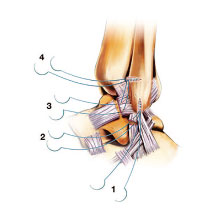
A Needle is Cut from each of the Sutures. This facilitates removal of the sutures and is safer for tying which is done by hand. The anchors are tested for purchase by pulling on the threads. Suture 2 is placed first. This allows delivery of the distal cuff into the incision. Its aim is to purchase part of the ATFL and CF ligament. Suture 1 purchases the CF ligament. Suture 3 is for the majority of the ATFL ligament. Suture 4 purchases the anterior portion of the ATFL and capsule and part of the extensor retinaculum. The sutures are then tied with the ankle in eversion from 1-4.